
Your billing team is working harder than ever. Your RCM director is fielding more denial appeals than last quarter. And your CFO is watching days sales outstanding climb while margins compress. The frustrating part? Most of this is preventable and the same problem looks different depending on where you sit.
For a Billing Manager, it’s a daily grind: eligibility mismatches caught too late, prior auth paperwork that takes hours, denials that come back weeks after submission with no clear root cause.
For an RCM Director, it’s a structural problem: denial rates trending upward year over year, staff burnout from repetitive rework, and payer rules that change faster than your team can track them.
For a CFO, it’s a margin problem: providers reporting that 10% or more of their claims are denied rose from 30% in 2022 to 41% in 2025, according to Experian Health’s State of Claims report. Reworking a single denied claim costs $25–$30 in staff labor alone and 65% of denied claims are never resubmitted at all, meaning most of that cost becomes permanent revenue loss.
AI-driven revenue cycle management addresses all three problems at once not by replacing your team, but by shifting when errors get caught. Rather than waiting for a payer to reject a claim and reworking it after the fact, AI evaluates eligibility, coding, and documentation before submission. Health systems deploying AI-driven revenue cycle solutions across eligibility, coding, and prior authorization are seeing cost-to-collect reductions of 30% or more, according to McKinsey’s analysis of full-scale AI deployment in the revenue cycle.
This article breaks down how that works and what it means for each person in the room when the decision gets made.
Why Denial Rates Keep Rising Even at Well-Run Organizations
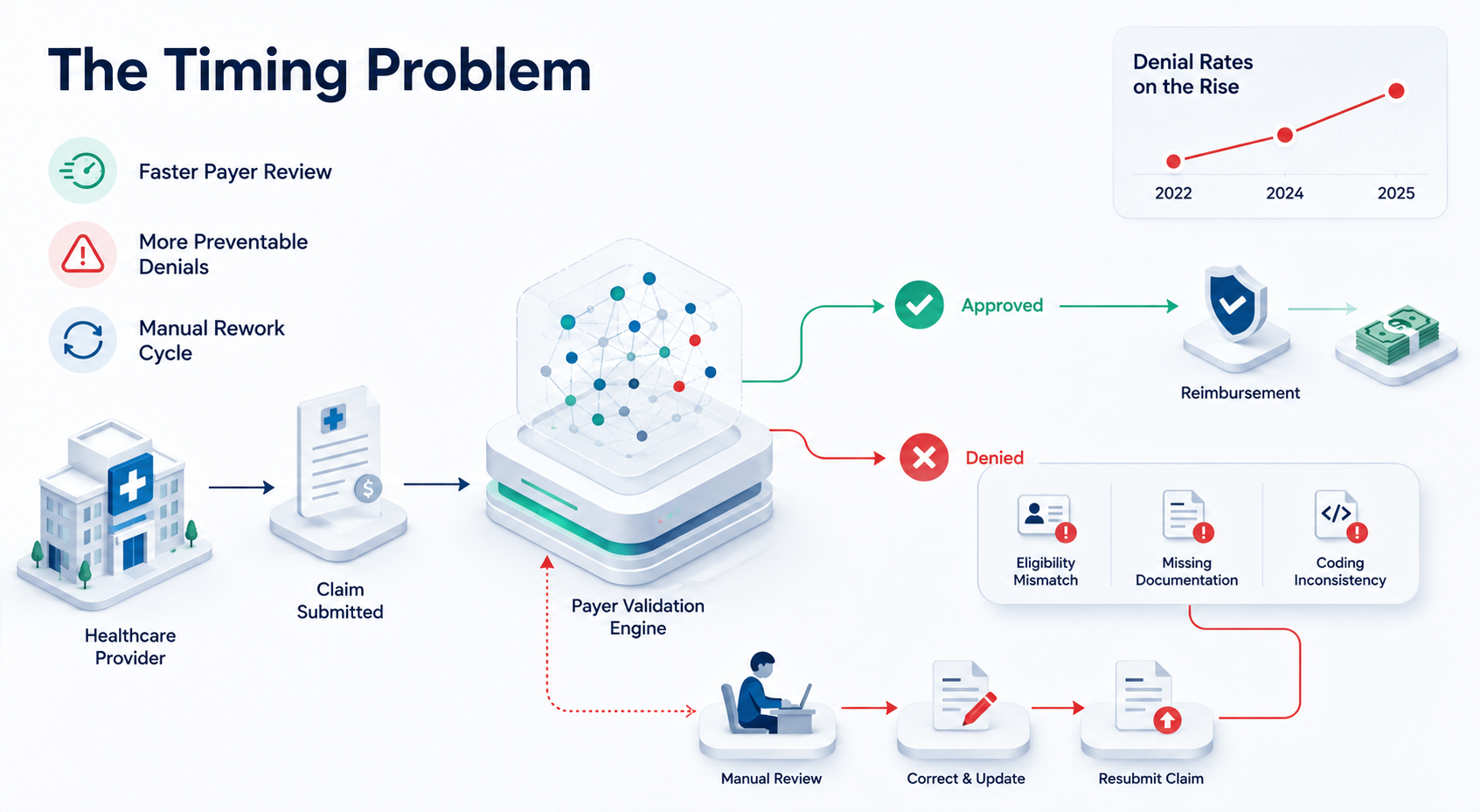
The denial problem looks like a billing problem on the surface. It isn’t. It’s a timing problem.
Most healthcare organizations catch errors after a claim has already been submitted which means after a payer has already reviewed it, flagged it, and issued a denial. The team then has to trace the root cause, correct it, resubmit, and wait again. Roughly 90% of denials are preventable, and nearly half originate in front-end functions like registration, eligibility verification, and authorization. The errors are fixable; they’re just being caught at the most expensive possible moment.
The trend is accelerating. Providers reporting that 10% or more of their claims are denied rose from 30% in 2022 to 38% in 2024 and 41% in 2025, confirmed by Experian Health’s State of Claims research. Meanwhile, 54% of providers report that claim errors are actively increasing, and 59% plan to invest in claims processing or denial reduction technology in the next six months. The market has reached an inflection point and a significant reason why is what payers are doing on their side.
The payer AI arms race most providers don’t talk about.
Payers have been deploying AI to review and deny claims at machine speed for several years. Their systems flag mismatches, identify documentation gaps, and issue denials in seconds. A Billing Manager reviewing the same claim manually cannot operate at that speed or scale. An RCM Director cannot build a team large enough to match algorithmic throughput with human effort. The result is a structural imbalance: algorithmic denials coming in faster than human teams can respond, appeal, and resubmit.
This is why denial rates are rising even at well-run organizations; it’s not a staffing problem or a training problem. It’s a speed and scale problem. The only viable response is AI on the provider side.
The financial data makes the stakes concrete. Reworking a single denied claim costs $25–$30 in staff labor alone, per MGMA and CAQH benchmarks. Inpatient denials now average $10,000 per claim. Outpatient denials average $825 per claim. And roughly 65% of denied claims are never resubmitted at all. That’s not rework cost, that’s revenue that disappears entirely.
How AI Fixes the Timing Problem, Before the Claim Reaches the Payer
The Old Way: Submit and Pray
Claims are coded, submitted, and the team waits — sometimes weeks — to find out whether a payer accepts, rejects, or requests more information. When a denial arrives, the rework cycle starts: trace the error, correct it, resubmit, wait again. For a Billing Manager, this means constant context-switching between new claims and denial queues. For an RCM Director, it means staff hours absorbed by work that should never have been necessary. For a CFO, it means cash sitting in limbo instead of posting to the ledger.
The New Way: AI as a Real-Time Audit Layer
AI-driven RCM evaluates each claim before it reaches the payer — checking eligibility, validating codes against current payer rules, and flagging documentation gaps in real time. The claim that reaches the payer portal has already passed a predictive denial-risk check. Errors get caught at the cheapest possible moment: before submission, not after rejection.
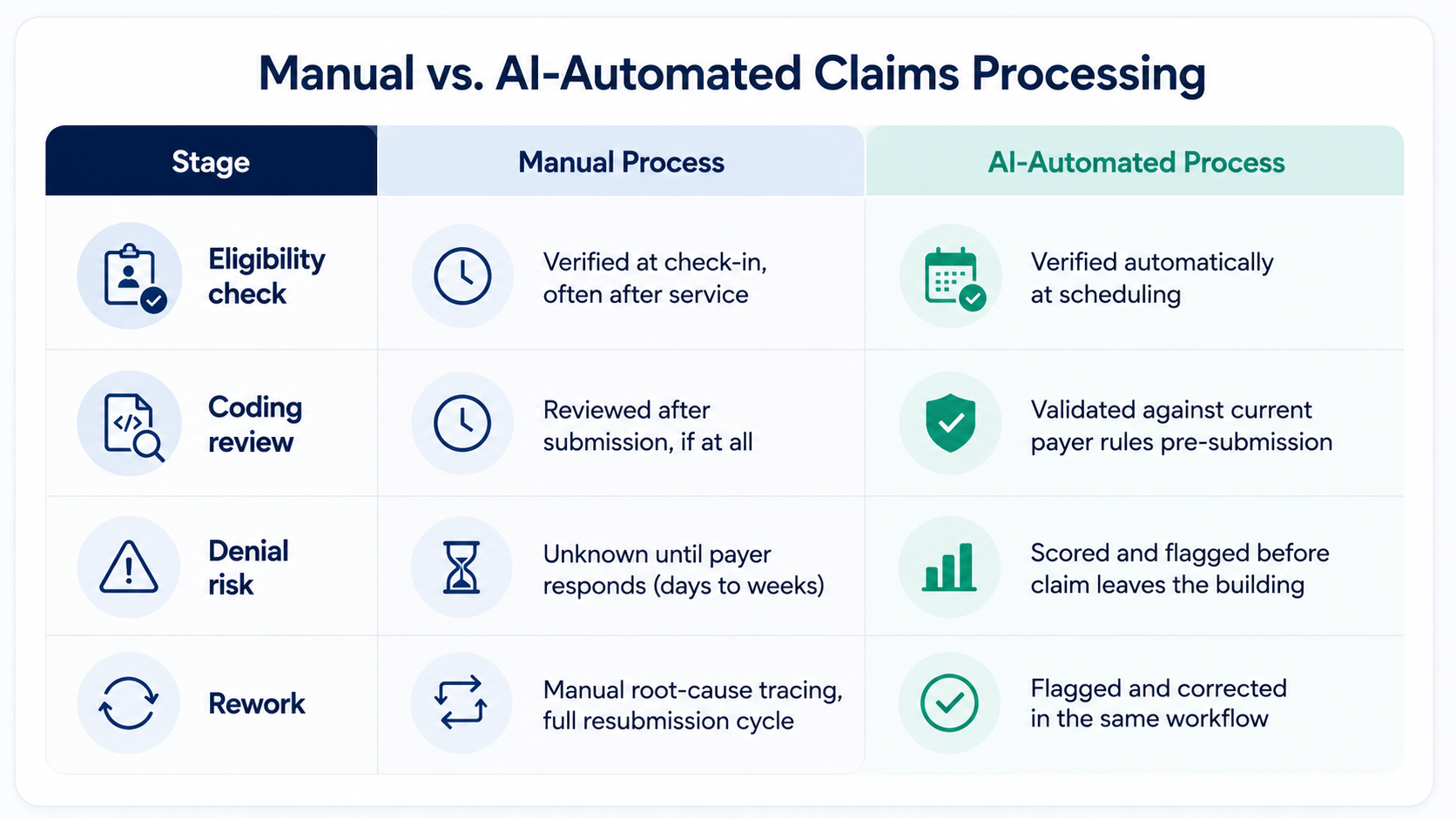
The savings come from preventing rework — not from doing the same rework faster.
What AI Actually Automates, The Three Functions That Drive Most Denials
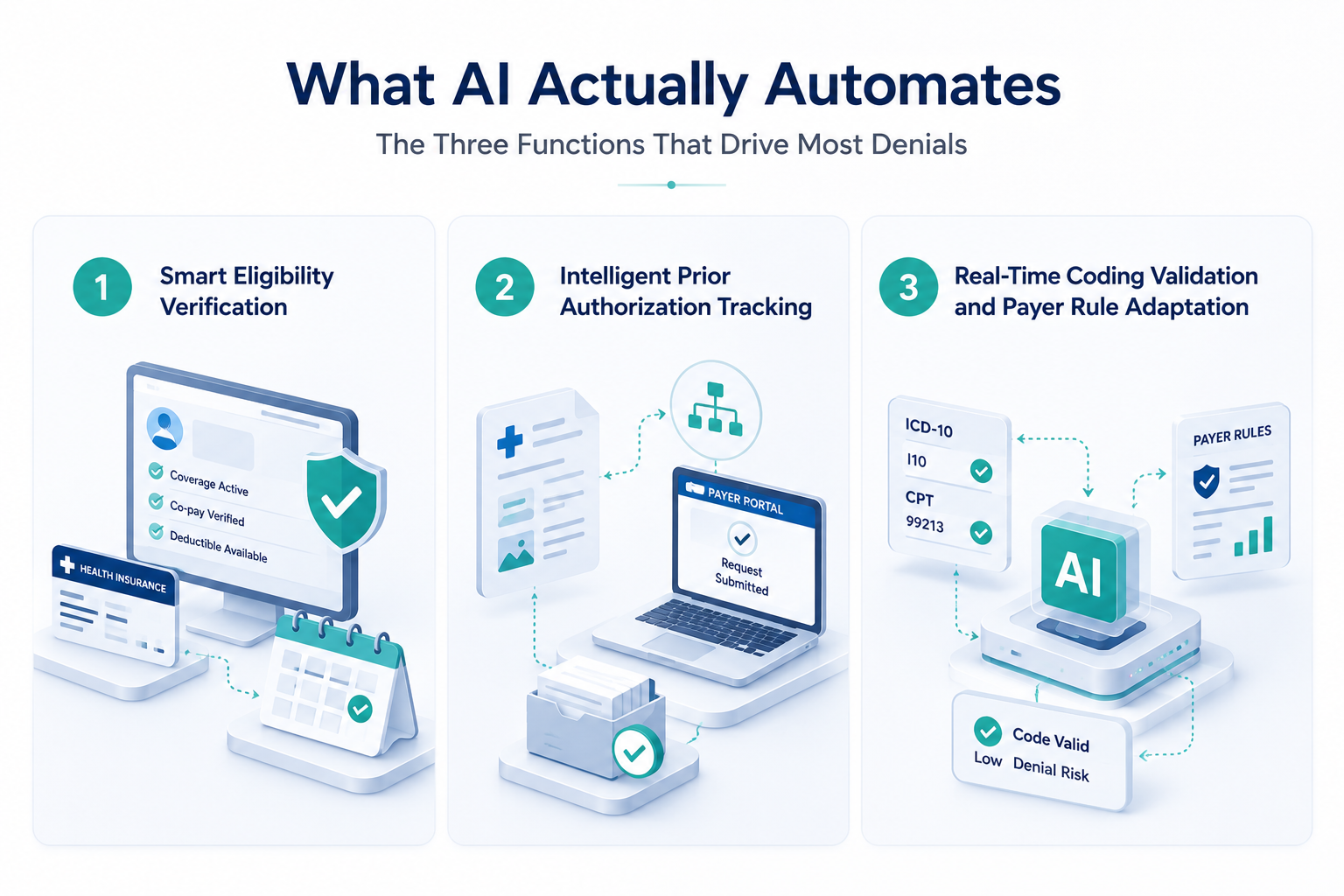
Pillar 1: Smart Eligibility Verification
Most front-end denials trace back to a single root cause: eligibility information that was either wrong or checked too late. AI verifies insurance coverage, co-pays, and deductibles automatically at the point of scheduling — not at check-in, not after the visit. For a Billing Manager, this eliminates one of the most common sources of same-day rework. For an RCM Director, it removes a denial category that should never exist. Real-time eligibility checks cross-reference coverage, coordination of benefits, and patient demographics in one workflow, catching mismatches before they ever become a claim.
Pillar 2: Intelligent Prior Authorization Tracking
Prior authorization is the bottleneck every RCM Director knows well — a process that requires staff to manually read clinical notes, match procedure codes, and submit authorization requests through payer-specific portals that change without warning. For a Billing Manager, it’s the task that takes the longest and yields the most unpredictable results. AI agents read clinical documentation, match it against current authorization requirements, and submit requests autonomously, removing the single largest source of delay in the prior-auth cycle.
Pillar 3: Real-Time Coding Validation and Payer Rule Adaptation
Payer rules change constantly — a code that was clean last quarter can trigger a denial this quarter if a payer policy shifted. Keeping up manually requires constant monitoring across dozens of payer portals, which no billing team can sustain at scale. Machine learning models trained on current payer rule sets flag mismatched ICD-10/ICD-11 or CPT codes before submission, adapting as payer policies change. For a CFO, this closes the fastest-growing denial category industry-wide. For an RCM Director, it removes the dependency on staff manually tracking payer rule changes.
Why This Doesn’t Require Replacing Your EHR, Or Disrupting Your Team
The most common hesitation from CIOs and RCM Directors: “What does implementation actually disrupt?” The answer is less than you’d expect — because AI doesn’t require replacing anything.
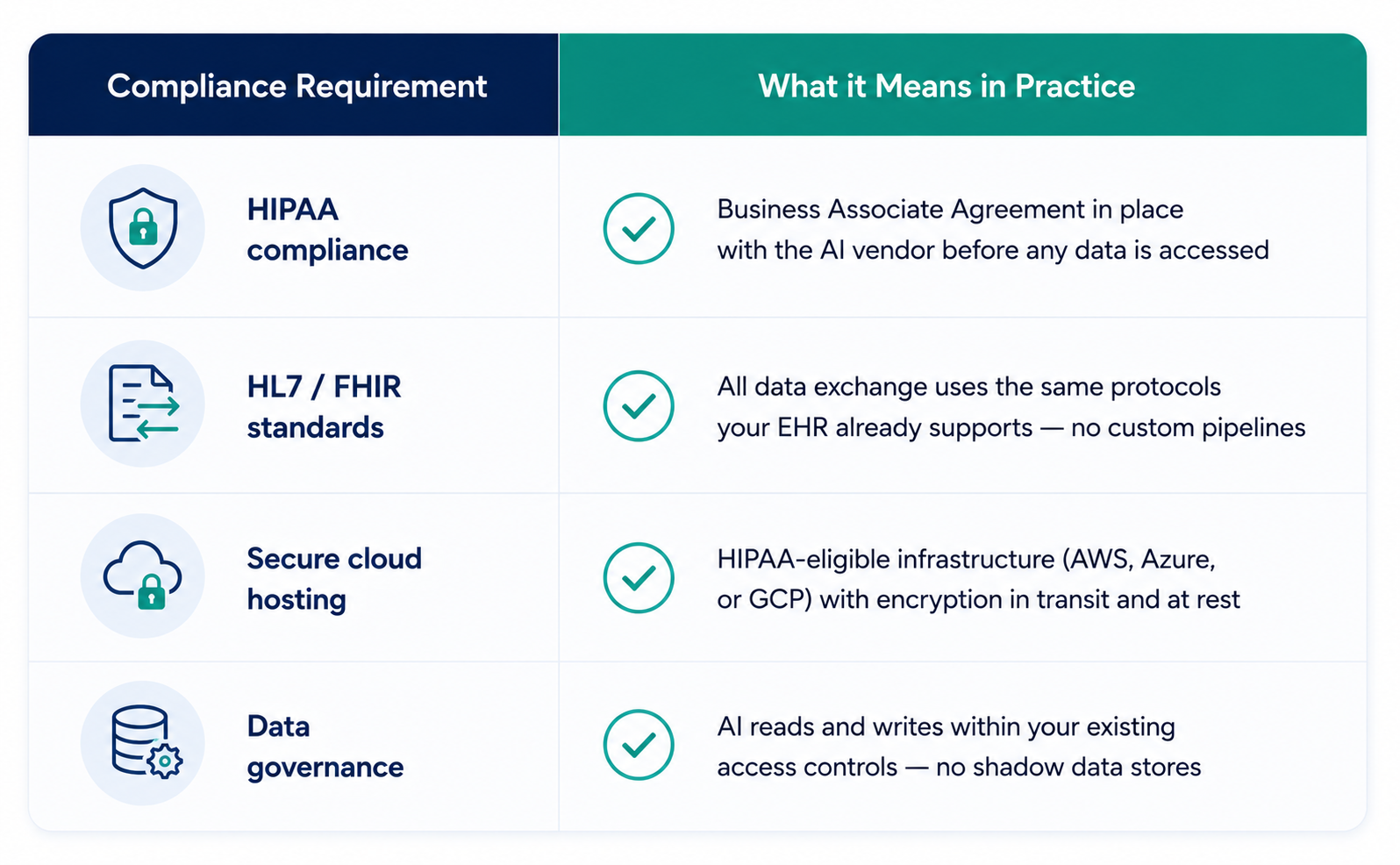
The AI integrates with what you already have — without modifying your core EHR codebase or requiring data migration. It reads clinical notes, updates patient statuses, and exchanges claims data through standard HL7 and FHIR APIs — the same integration layer your systems already use to communicate with each other. Your EHR configuration stays intact. Your billing platform stays intact. The AI operates through the front door, not around it.
Think of it less like a transplant and more like adding a translator that makes your existing systems faster and smarter — one that works through standard protocols your IT team already governs.
What that means for your team in practice:
- Your Epic, Cerner, Meditech, or Athenahealth instance stays exactly as configured — no codebase changes, no version conflicts
- Clinical notes and patient data are accessed via read/write API calls, not extracted into a separate system
- No data migration, no retraining on a new platform
- Implementation happens in the background — your billing team keeps working throughout
- HIPAA compliance is maintained — the AI operates within your existing data governance structure, not around it
Compliance by design, not afterthought. Any AI tool touching patient claims data needs to meet the same bar your EHR does — and the compliance obligations for healthcare AI extend beyond HIPAA to cover FDA’s Software as a Medical Device framework and, for organizations with European exposure, the EU AI Act.
Organizations that treat the AI layer as part of their compliance perimeter from day one — not as a tool bolted on after the fact — get the most value from implementation and avoid the compliance retrofitting that delays ROI.
What a 30% Denial Reduction Actually Looks Like, For Each Person in the Room
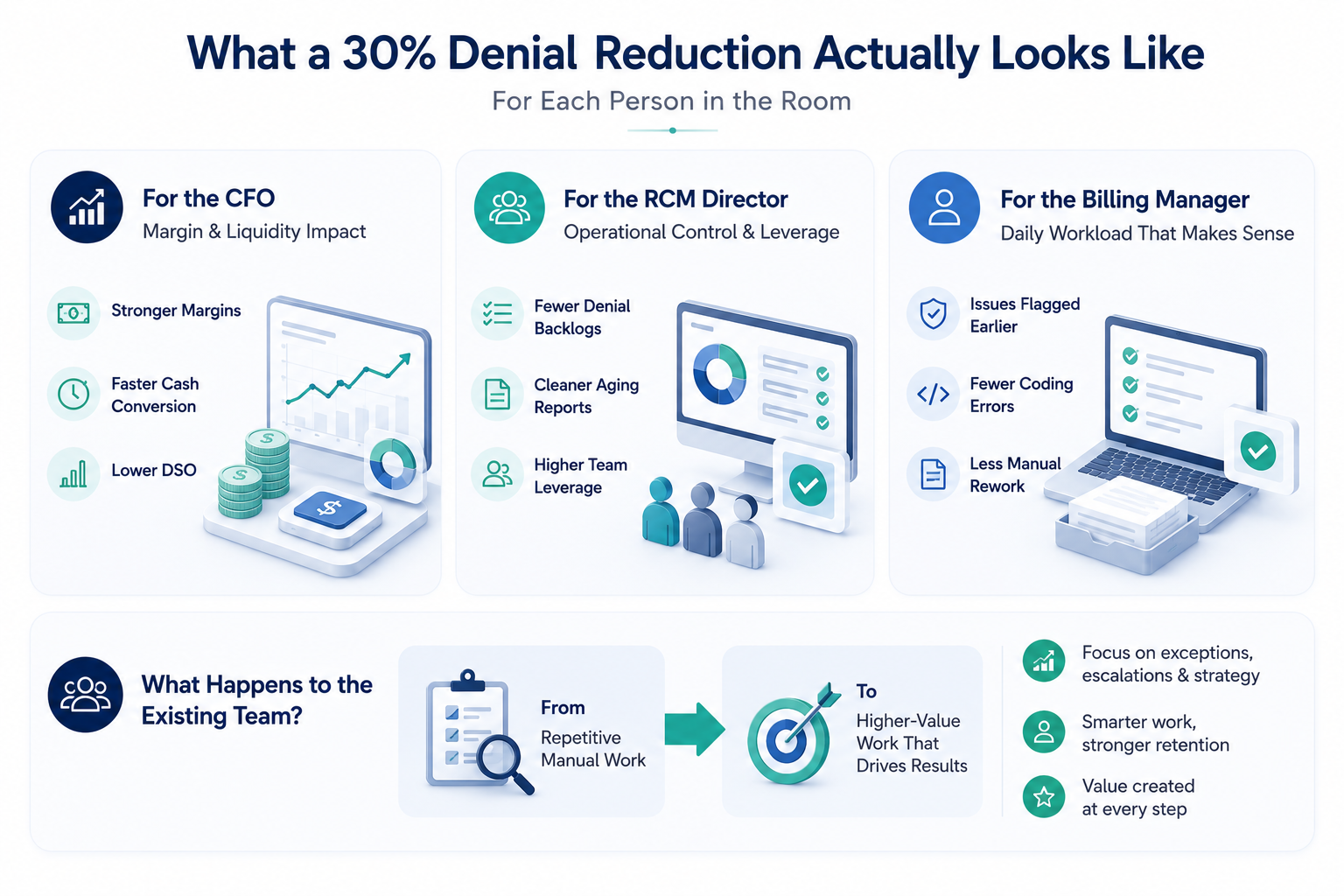
Reduced denials and faster prior authorization show up differently depending on who’s measuring them.
For the CFO: margin and liquidity metrics.
Higher first-pass clean claim rates mean fewer claims sitting in a denial-and-appeal loop. Cash that used to take 60+ days to collect moves through the cycle faster, reducing days sales outstanding. EY’s healthcare revenue cycle research confirms this: AI-enabled RCM models convert work performed into cash more consistently and predictably. McKinsey’s 30–60% cost-to-collect reduction range reflects the compounding effect of AI across the full claims lifecycle — not just one function. For a more granular breakdown of documented ROI from healthcare AI deployments across clinical documentation, imaging, and billing, the numbers are now verifiable, not projected.
For the RCM Director: operational control and staff leverage.
When AI handles eligibility checks, coding validation, and payer portal status lookups, your team shifts from reactive rework to proactive denial prevention. RCM Directors who have made this shift report fewer denial backlogs, cleaner aging reports, and billing teams that spend their time on complex appeals and payer strategy rather than chasing basic errors. The denial overturn rate improves because staff are focused on cases that actually require human judgment — not the ones that could have been prevented at scheduling.
For the Billing Manager: daily workload that makes sense.
The most immediate change is what doesn’t land on the billing desk. Eligibility mismatches flagged before the visit. Coding errors caught before submission. Prior auth submissions handled without manual portal navigation. The rework queue shrinks not because the team is working faster, but because fewer errors are making it to the payer in the first place. For a team that’s been running at capacity on preventable denials, that’s a meaningful shift in daily work.
What happens to the existing team?
If AI handles the routine work, what happens to the staff doing it now? Headcount doesn’t necessarily decrease — but its composition shifts. Staff spending 60–70% of their time on eligibility checks, portal lookups, and basic rework move to exception handling, payer escalations, and denial pattern analysis. The team gets smaller only through attrition, not displacement — and the work they’re doing is higher-leverage. That’s a retention argument as much as an efficiency one.
Why the Window to Act Is Narrowing, And What to Do Next
The competitive dynamic has shifted permanently. Relying on manual human review puts providers at a severe structural disadvantage against payers who use sophisticated algorithms to reject submissions instantly. This automation imbalance—not a drop in staff performance—is driving the current surge in industry-wide denial rates.
The market is responding rapidly. Experian Health reports that 59% of providers plan to invest in denial reduction technology within the next six months. Early adopters are building institutional AI capabilities today, while those who delay will absorb rising permanent revenue losses and unsustainable manual labor costs.
JanBask bridges this gap through a seamless five-stage framework spanning Discovery, Architecture, Implementation, Validation, and Ongoing Compliance Monitoring. This methodology protects your existing EHR investments while adapting to shifting regulations, a process explored deeper in our AI infrastructure guide.
Whether you are a CFO managing liquidity, an RCM Director seeking operational leverage, or a Billing Manager fighting daily backlogs, the critical question is no longer if you should adopt AI, but where to begin.
Book a Free Revenue Cycle Workflow Audit today. We will analyze your current EHR environment and denial patterns to pinpoint exactly where AI will deliver your fastest financial return.
Ready to accelerate your Artificial intelligence journey?
Talk to a JanBask specialist and get a strategy session tailored to your business.



