
As of 2026, the U.S. Food and Drug Administration has cleared over 1,451 AI-enabled medical devices for active use in hospitals and clinics. This is not a forecast. These tools are running right now, reading scans, writing clinical notes, processing insurance claims, and flagging patients at risk.
An AI agent in healthcare is a software system that can take in data, make a decision, and act on it, without waiting for a human to tell it what to do at every step. It is different from a simple automation tool because it learns, adapts, and handles complex tasks across the care workflow.
This blog covers four things every healthcare and health-tech leader needs to know: where AI agents are genuinely deployed today, what compliance rules apply, what financial returns real organizations are seeing, and what you need to get right before you go live.
Where AI Agents Are Actually Being Used Today
Most conversations about AI in healthcare talk about what the technology will do. This section focuses only on what it is doing right now, in live clinical and operational settings.
Clinical Documentation
Physicians in the United States spend close to two hours on paperwork for every one hour they spend with a patient. Ambient AI scribes are changing that. Tools like Nuance DAX and Abridge listen to a doctor-patient conversation and automatically generate a structured clinical note for the physician to review. A study published in JAMA Health Forum in January 2026 found that after 30 days of using an ambient AI scribe, the share of clinicians reporting burnout dropped from 51.9% to 38.8%. Health systems across the U.S., U.K., and Singapore have already moved this from pilot to standard practice.
Medical Imaging and Diagnostics
Radiology is where AI has the deepest footprint in healthcare today. Over 900 FDA-cleared AI tools are currently authorized for reading CT scans, MRIs, X-rays, and ultrasounds. These tools work inside existing radiology workflows at major hospital networks, flagging findings for radiologist review rather than replacing the specialist. The result is faster turnaround on reports and a meaningful reduction in missed findings at the screening stage.
Prior Authorization and Revenue Cycle
Prior authorization, the process of getting insurance approval before a procedure, is one of the most time-consuming administrative tasks in healthcare. AI agents now handle this end to end. They check the payer’s requirements, fill out the request, and submit it automatically. What used to take eight to ten days is being completed in 24 to 48 hours at health systems that have deployed these tools. On the billing side, AI agents review clinical notes, suggest the correct billing codes, and check claims against payer rules before submission, reducing rejected claims and speeding up revenue recovery.
Remote Patient Monitoring
Millions of patients now use connected devices at home, blood pressure monitors, glucose trackers, pulse oximeters, and smartwatches, that send a continuous stream of health data. No care team can manually review all of that data for thousands of patients at once. AI agents solve this by watching the incoming data around the clock and alerting the care team only when a reading crosses a clinically meaningful threshold. For heart failure patients specifically, this approach has been associated with an 18 to 25% reduction in hospital readmissions within 30 days, according to research published in NEJM Catalyst.
Compliance – The Three Rules You Cannot Skip

Deploying AI in a healthcare setting is not the same as deploying it in retail or finance. Patient data is involved. Clinical decisions are involved. That means the legal responsibilities are significant, and the cost of getting it wrong is high. There are three frameworks every team must understand before going live.
HIPAA: Protecting Patient Data in the United States
Any AI tool that touches patient health information in the U.S. must comply with the Health Insurance Portability and Accountability Act, commonly known as HIPAA. The rules are specific. Every vendor that handles patient data must sign a Business Associate Agreement before they are given any access, no exceptions. AI agents must only access the minimum amount of patient information needed to complete their task. Every action the system takes involving patient data must be logged and stored for at least six years under the HIPAA Security Rule. If a data breach occurs, even an accidental one, the organization is legally required to notify the affected patients. According to IBM’s 2025 Cost of a Data Breach Report, the average cost of a healthcare data breach is $7.42 million. That figure alone makes compliance a financial priority, not just a legal one.
FDA’s Software as a Medical Device Framework
The U.S. Food and Drug Administration classifies certain AI tools as medical devices. If an AI agent directly influences a clinical decision, such as recommending a diagnosis or suggesting a treatment plan, it almost certainly requires FDA clearance before it can be used in a clinical setting. The standard pathway is a 510(k) submission, though some novel tools go through the De Novo process. Tools that provide general background information, where the clinician makes the final call independently, may fall outside this requirement, but that determination must come from a formal legal review, not an assumption. Once a tool is cleared, the obligation does not end. The organization must monitor the system for accuracy issues, report significant malfunctions to the FDA, and follow a pre-approved update plan, particularly important for systems that continue learning from new data.
The EU AI Act: For Any Organization Operating in Europe
If your organization operates in Europe or serves European patients, the EU AI Act now applies to you. Healthcare AI is classified as high risk under the Act’s Annex III, which triggers a defined set of obligations. A full safety and compliance assessment must be completed before the system goes live. The system must be registered in the official EU AI database prior to market entry. Human oversight mechanisms must be in place so that errors can be caught and corrected before they affect patients. Patients also have the right to request an explanation of any AI-driven decision that significantly affects their care. Fines for non-compliance can reach €30 million or 6% of global annual revenue, whichever is higher.
The practical takeaway across all three frameworks is the same: classify your AI tool’s regulatory category before procurement, not after deployment. Retrofitting compliance is far more expensive than building it in from the start.
What ROI Actually Looks Like, With Honest Numbers
For a long time, the financial case for healthcare AI was built on projections. That has changed. Health systems that deployed carefully, measured honestly, and scaled what worked are now reporting verified returns across multiple areas of operation.
The table below reflects documented outcomes from independent research and industry audits, not vendor claims.
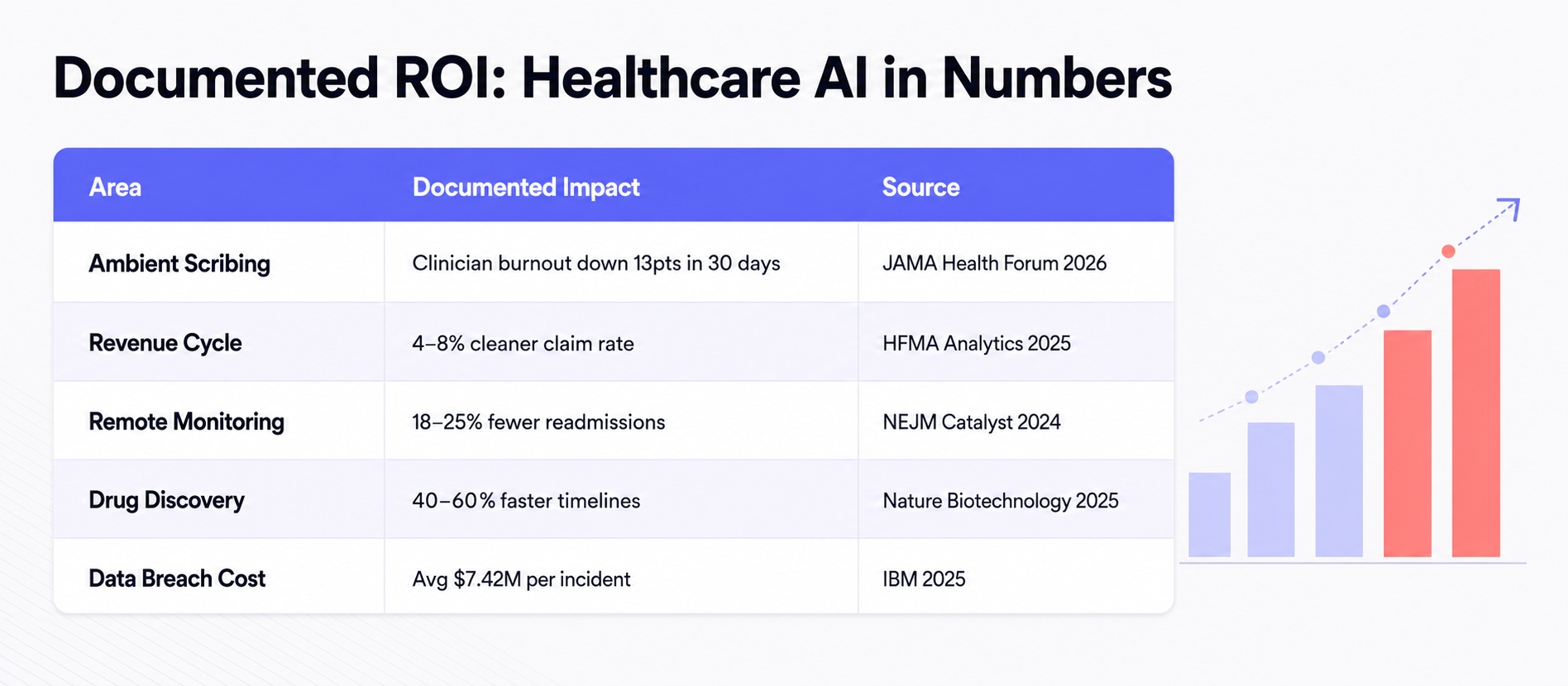
What these numbers show is that the returns are not uniform and they do not all arrive at the same time. Organizations that set realistic expectations by area see far better outcomes than those chasing a single headline ROI figure.
A practical way to think about the timeline is in three stages. In the first three to six months, the gains are primarily operational, time saved on documentation, faster claim submissions, reduced administrative back-and-forth. Between six and twelve months, revenue cycle improvements begin to show up in clean claim rates and reduced denials. Clinical outcomes, reductions in readmissions, adverse events, and diagnostic errors, typically take nine to eighteen months to surface in the data, because they require enough patient volume and follow-up time to be statistically meaningful.
The most important discipline in measuring ROI is also the simplest one: record your baseline before you go live. Without a clear picture of where things stood before the AI was deployed, it is impossible to prove what changed because of it. Organizations that skip this step often find themselves unable to justify continued investment, not because the tool failed, but because they have no way to show that it worked.
What to Get Right Before You Deploy

Understanding the use cases and the financial returns is only half the work. The organizations that consistently get the most out of healthcare AI are the ones that invest in internal readiness before a single system goes live. These are the five areas that matter most.
Start with your data infrastructure
AI agents are only as capable as the data they can access. If patient records are fragmented across disconnected systems, or if data quality is inconsistent, the agent will produce unreliable outputs regardless of how sophisticated the underlying model is. Before evaluating any AI tool, audit whether your existing data systems can support it.
Define what success looks like, and measure where you start
Every deployment needs a clear success metric tied to a specific workflow. Is the goal fewer rejected claims? Shorter documentation time? Fewer readmissions? Whatever it is, record the baseline number before go-live. Without it, you cannot demonstrate value to leadership or justify the next phase of investment.
Begin with one high-volume, low-risk workflow
The worst place to start is a high-stakes clinical decision like diagnosis or medication dosing. The best place to start is a workflow that is repetitive, well-defined, and high in volume — prior authorization processing, appointment scheduling, or clinical note drafting are all proven entry points. Early wins in lower-risk areas build the organizational trust needed to move into more complex territory.
Assign a human review checkpoint for every high-stakes output.
AI agents should escalate to a clinician whenever they are not sufficiently confident in their output, and every consequential decision — medication changes, triage prioritization, discharge planning — must have a human in the loop. This is not just good practice. Under both HIPAA and the EU AI Act, it is a compliance requirement.
Test for bias before and after deployment.
AI systems can perform well on average but poorly for specific patient groups — elderly patients, non-English speakers, and historically underrepresented communities are the highest-risk segments. Bias testing should happen before launch and at regular intervals afterward. A system that works well for 80% of your patient population but fails the remaining 20% is not a safe system.
What Comes Next
The evidence is no longer theoretical. With over 1,451 AI-enabled medical devices cleared by the FDA, ambient scribes reducing clinician burnout in live hospital settings, and revenue cycle tools recovering millions in previously lost claims, healthcare AI has moved well past the pilot stage. The organizations seeing the strongest results are not the ones that moved the fastest, they are the ones that built the right foundation first.
That foundation comes down to three things: clean, connected data that AI agents can actually work with; compliance frameworks put in place before deployment, not after a problem occurs; and a disciplined approach to measuring outcomes from day one.
For healthcare organizations that are ready to move from evaluation to execution, the next step is finding an implementation partner who understands both the clinical environment and the technical requirements.
JanBask’s AI Consulting Services & JanBask’s AI Integration Services help healthcare and health-tech organizations design, deploy, and govern AI systems that are built to work in regulated, high-stakes environments, not just in a demo.
The technology is proven. The financial case is clear. What comes next is execution.
Ready to accelerate your Artificial intelligence journey?
Talk to a JanBask specialist and get a strategy session tailored to your business.



